When Okon Emannuel, 56, fell ill in June 2021, he visited a local chemist (drug store) four blocks from his residence in Midim, Abak Local Government Area of Akwa Ibom State.
“I think it was malaria. But after taking the tablets the chemist mixed for me, I still felt fever(ish) again,” he said.
As his situation got worse, he sought care at “Polyclinic” – the Primary Healthcare Centre (PHC) Operational Base – situated some three kilometres away, despite the existence of the Midim PHC in his community.
Mr Emmanuel said his preference for Polyclinic is shared by many other residents of the area. “The one you talk about (Midim PHC); how many people go there that time?” he asked.
“Maybe pregnant women for antenatal,” a woman, who had been listening to the conversation quickly added. “Many people here go to Polyclinic, because it is better,” Mr Emmanuel said.
The low patronage at PHC Midim was not unconnected with its dilapidated state at the time. According to a 2021 assessment report by UDEME, a social accountability initiative of the Centre for Journalism Innovation and Development, the PHC had broken ceilings, crumbling roofs and doors and windows affected by termite infestation.
However, this is not the situation at PHC Midim today courtesy of the Nigerian government’s intervention through the Basic Healthcare Provision Fund (BHCPF). A visit to the PHC in August showed that it had been renovated and repainted.
“The fund has helped to transform this place. We have replaced the doors and the wood in the ceiling that were destroyed by termites and fumigated the place from the ceiling up and down,” Itohowo Duncan, the officer in charge of the PHC, told PREMIUM TIMES. “We have more patients coming in here now than before.”
A generator was also procured to provide power supply at the PHC, putting an end to the long years of borrowing the village head’s generator.
Sylvester Ibanga, the village head, was full of praise for the federal government’s intervention.
“It has helped to improve the health centre a lot. They were able to repair a lot of things in the place. They even procured a generator to fix the electricity and water issues there. We are happy and we thank the government for this project,” he said.
About BHCPF
The Nigerian government introduced BHCPF under the National Health Act (NHAct) 2014 to provide free minimum basic healthcare to the most vulnerable populations through PHCs across Nigeria and reduce personal out-of-pocket payments and associated financial risks, through health insurance.
The initiative is funded with a minimum of one per cent of the Consolidated Revenue Fund (CRF), grants from international partners and other donors. The fund is disbursed via three gateways: 50 per cent for the provision of Basic Minimum Package of Health Services (BMPHS) to citizens via the National Health Insurance Scheme (NHIS), five per cent for treatment of medical emergencies and 45 per cent to improve PHCs’ service delivery through the National Primary Health Care Development Agency (NPHCDA).
Of the 45 per cent, 20 per cent is for the provision of essential drugs, vaccines and consumables for eligible PHCs, 15 per cent is for the maintenance of PHC facilities and equipment and 10 per cent is for the development of PHC staff.
For the NHIS Gateway, citizens and healthcare providers are expected to be enrolled as beneficiaries of the BHCPF, to enable them to access preventive, protective, promotive, curative, and rehabilitative health services at designated PHCs. However, these health services shall be funded through the State Health Insurance Agencies and State Health Insurance Schemes (SHIA, SHIS), at an agreed premium.
In 2018, President Muhammadu Buhari flagged off the Basic Health Care Provision Fund (BHCPF) with an appropriation of N55.1 billion from the Consolidated Revenue Fund (CRF), in addition to $2 million from the Bill and Melinda Gates Foundation, $20 million from Global Financing Facility (GFF) and £50 million donated by the Department for International Development (DFID) to cover 2018 – 2023.
Multiple reports had previously documented the decrepit conditions of PHCs across the state, citing insufficient drug supplies, understaffed, ill-equipped and dilapidated facilities, occasioned by neglect, lack of political will and poor health financing.
However, following the launch of the BHCPF in Akwa Ibom in the second quarter of 2021, and subsequent disbursement of funds in 2022, PREMIUM TIMES’ visit to Essien Udim, Uruan, Abak, Eket and Esit Eket council areas, revealed that PHCs have been revitalized, particularly with regards to the rehabilitation of previously dilapidated structures and facilities.
PREMIUM TIMES gathered that a total of 231 PHCs had benefited from the fund, each receiving around the sum of ₦611,000. PREMIUM TIMES observed that all beneficiary PHCs had been renovated and repainted; each spotting uniform yellow and green colours.

At PHC Nwaniba in Uruan LGA, the bad doors and windows have been replaced while the building has been repainted and the borehole repaired. A member of staff, Mfon Charles, commended the government for introducing the scheme.
“The doors and windows which were bad before have been changed and the borehole that was not working before,” she said. “As you can see, the building was also repainted to make it look better.”
The Fund served a similar purpose at PHCs in Ekpene Ibia and Ndon Ebom, covering the cost of painting, repair of ceilings that were previously falling off and replacement of wooden doors and windows with metal ones to improve security at the facilities. It also facilitated the purchase of a Sumo pump and a new signpost at PHC Ekpene Ibia.

“The fund we got has really helped to fix many of our needs here. Like the former door that fell off one morning after I had night delivery, we have changed it and others to iron doors which are more durable to protect the vaccine cooler, solar batteries and freezer from theft,” Anthonia Attah, who heads the facility, said.
Before the advent of the BHCPF, only the PHC Adiasim was in good shape in Essien Udim LGA, having been demolished and rebuilt to standard by a philanthropist in the community, Oliver Ebong, in 2018. Mfonobong Sam, the OIC of the PHC, said she did not have full knowledge of how funds from the BHCPF were utilised as she was “just posted there in March 2022.”
The BHCPF is also responsible for the recent renovation of the previously dilapidating structures at PHC Odoro Ikot I and II – the other beneficiary PHCs in the Essien Udim LGA. Catherine Icho, the OIC, thanked the government for the initiative, adding that it had improved conditions at the facility.

“If you see this health centre before, the roof was leaking and falling off. I used the money to buy zinc, ceiling and the new doors,” she said.
She lamented the shortage of staff, and lack of water and power supply at the facility and appealed to the Rural Electrification Agency (REA) to repair the solar-powered generator it donated to the facility.
In Abak LGA, BHCPF has equally brought succour to beneficiary-PHCs. At the operational base, Ime Udo, the monitoring and evaluation officer, commended the government for the Fund, saying it has improved the condition of many of the PHCs. He however added that “more needs to be done.”
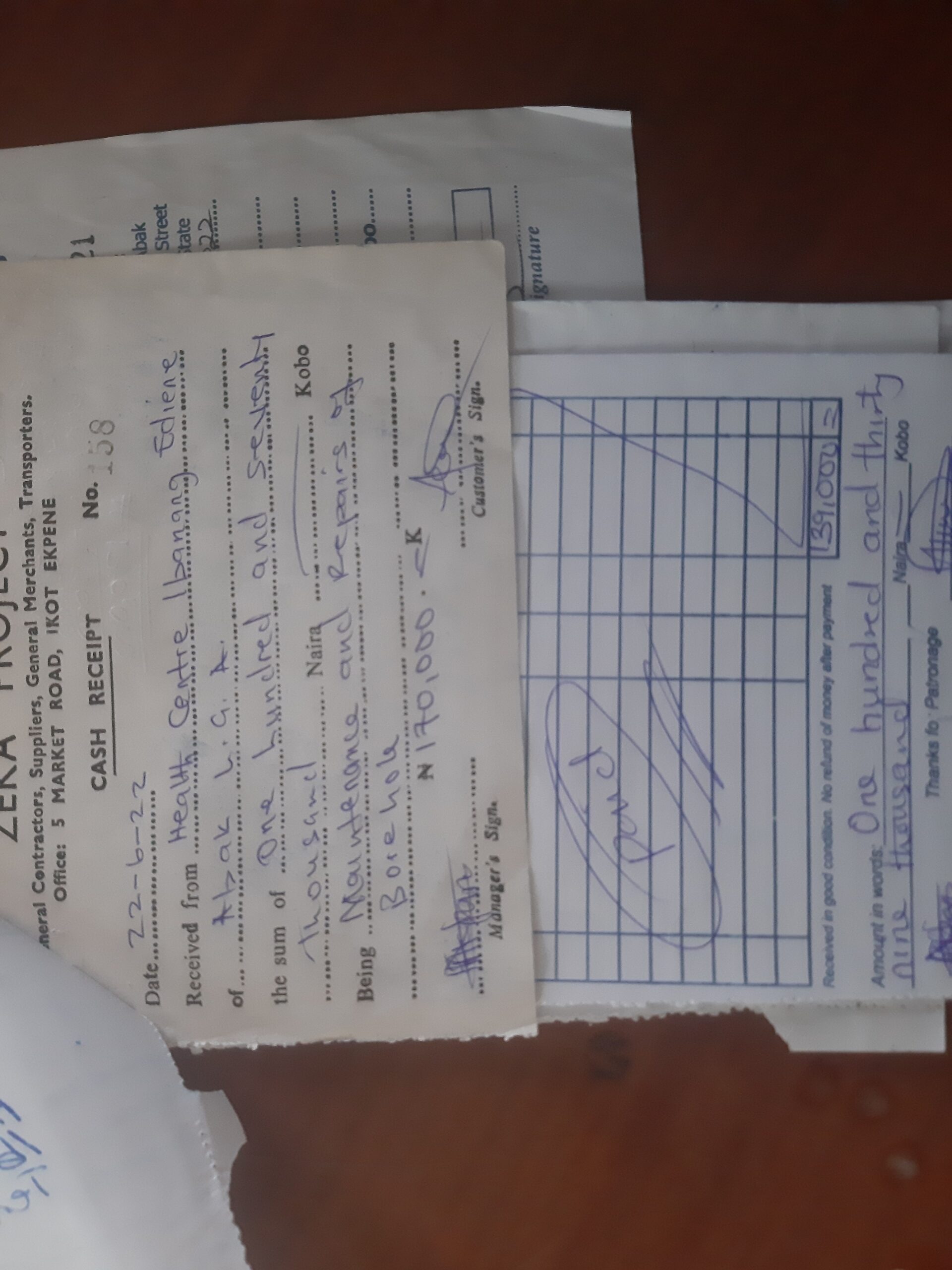
Blessing Ime, who used to attend antenatal care at PHC Ibanang Ediene, was delighted by the renovation of the PHC.
“Before now, we could not use the toilet but now they have repaired it,” she said. The broken roofs and ceilings have also been replaced, courtesy of the BHCPF.

The head of the facility at PHC Midim, Itohowo Duncan, was also full of praise for the BHCPF. Through the Fund, the facility, which had been ravaged by termites, had been rescued.
“The fund has helped to transform this place. We have replaced the doors and the wood in the ceiling that were destroyed by termites and fumigated the place from the ceiling up and down,” she said. A generator was also purchased to provide power supply at the PHC, putting an end to the long years of borrowing the village head’s generator.

There were signs of recent renovations at PHC Afaha Obong, including the newly installed gate, windows, iron doors, ceilings and electrical equipment. The OIC, Mfon Nseyo, said “the fund has assisted in rehabilitating the PHC.”
From Ikot Okudomo to Ikot Ukpong, Mkpok and Afaha Atai, there are tales of rehabilitation of PHCs in Eket LGA, courtesy of the BHCPF.
Nwaiwu Florence, a patient at PHC Idua in Eket LGA, acknowledged recent changes at the facility courtesy of the BHCPF intervention.

“The last time I was here for my vaccine last year, this place was not like this. I noticed that the broken floors, bad roof, doors and windows have been worked on. They have also purchased more seats,” she said.
At the PHC Idung Iniang, the OIC, Mfon Batta, urged the government to sustain the project so that some of the challenges facing the facilities can be a thing of the past.

“This is the first renovation of this PHC since it was built. If they can continue like this before you know, many of the issues we have been having will be solved,” she said.
The story is no different for PHCs in Esit Eket LGA. PREMIUM TIMES found that all the beneficiary-PHCs had received various levels of renovation, and could be easily identified by their recently painted yellow and green walls.
The PHC in Etebi was doubly lucky. A new building was recently constructed by a former Minister of the Niger Delta, Godswill Akpabio, but the old building in the facility also got renovated through the BHCPF.
Charlie Hannah, the head of the facility, said the PHC had been selected as a beneficiary of the BHCPF “before the new building was constructed by the minister.”
Unlike many of its kind, the PHC has water and power supply, just like the PHC in Iko-Effak Akpautong, another beneficiary of the BHCPF.
Apart from the renovation of the building and purchase of furniture, a new generating set was recently purchased for the PHC Ikpa Town. According to the OIC, Ekaette Bassey, the decision to make the purchase was made to tackle the facility’s long-drawn challenge with irregular power supply.
Findings by PREMIUM TIMES revealed that the development strides at the PHCs are a product of the synergy with their respective Ward Development Committees (WDCs) – a group of community members selected to support the heads of the PHCs in the administration of the Fund.
There is also a culture of record-keeping for accountability by the heads of the PHCs. Each maintains a folder where all documents – including payment receipts, pictures of the PHC’s previous condition and bank statements – are kept.
Controversies over beneficiary PHCs selection
Meanwhile, the selection of the PHCs to receive the funds in the state sparked controversies, stemming from the inequitable distribution of beneficiary PHCs across the LGAs. PREMIUM TIMES gathered that some LGAs received more beneficiaries than others.
In Uruan LGA, for instance, only three out of nine PHCs were selected to receive funding. Of the 19 PHCs in Essien Udim LGA, only three were selected, and 10 out of 14 PHCs were selected in Abak LGA. In Eket LGA, 11 of the 15 PHCs benefited from the Fund, just as nine out of the 13 PHCs in Esit Eket LGA were selected.
The criteria employed in the selection of beneficiaries remain a mystery to the public.

“It is unfortunate. Here in Essien Udim, only three out of almost 20-something facilities were selected. So, I wonder what criteria they used in selecting the facilities. How come other local governments have more beneficiaries and we have just three?” a nurse working in one of the PHCs queried.
There are also concerns that some dilapidated PHCs critically in need of intervention, were left out.
A visit to the non-beneficiary PHCs across the five LGAs revealed that most of the facilities are grossly understaffed, ill-equipped and dilapidated.
Facilities like PHC Mkpatak and the PHC Operational Base, Ikot Ebak in Essien Udim LGA, reek of dilapidation and long years of neglect, especially PHC Ekpenyong II which is totally in shambles. The ceilings at the PHC had crumbled, forcing staff and even patients who were receiving treatment, to always run for cover.

In Abak LGA, the ceilings of many of the wards and offices at the PHC Operational Base are prevented from crumbling with the support of sticks, just as the health post at Abak Itenge requires urgent intervention.
There is a need to provide intervention for PHCs in Esit Urua and Ikot Abia in Eket LGA, which operate from single classrooms in schools – Apostolic High School Esit Urua and Government Primary School Ikot Abia, respectively.
Others requiring attention also include the PHCs Odoro Nkit, Ntak Inyang and Akpasong in Esit Eket LGA.
Apart from the issue of structural deficiency observed, many of these PHCs are also plagued with a shortage of drug supplies. When they can, PHC staff stock up the pharmacies with drugs and essentials from their personal pockets, in a bid to make the drugs readily available for patients at a cost. Apart from availability, patients who spoke with PREMIUM TIMES said it saves them the risk of buying counterfeit drugs.
“Most times it is better to buy the drugs at the health centre because you are sure that it is original instead of going by yourself to the chemist or pharmacy and buying fake,” Esther Monday, a patient, said.
The situation is the same across the state. Apart from antimalarial drugs and antiretrovirals (ARVs), patients bear the costs of drugs and other medical treatments, despite the implementation of the Basic Healthcare Provision Fund (BHCPF) in the state.

PHCs’ task of revenue generation
Despite efforts to improve rural healthcare with initiatives like the BHCPF, findings by PREMIUM TIMES revealed that PHCs across the state are tasked to generate and remit revenues by LGA councils.
Councils maintain revenue registers at every facility, with which PHC staff are mandated to record the details of every patient and the fees collected. Charges differ across LGAs. At PHCs in Uruan LGA, adults pay ₦100, children ₦50, while pregnant women pay ₦100 and ₦200 after delivery. It is slightly different for PHCs in Essien Udim LGA, where pregnant women pay ₦500 before and after delivery, and Eket LGA, where adults are charged ₦50.
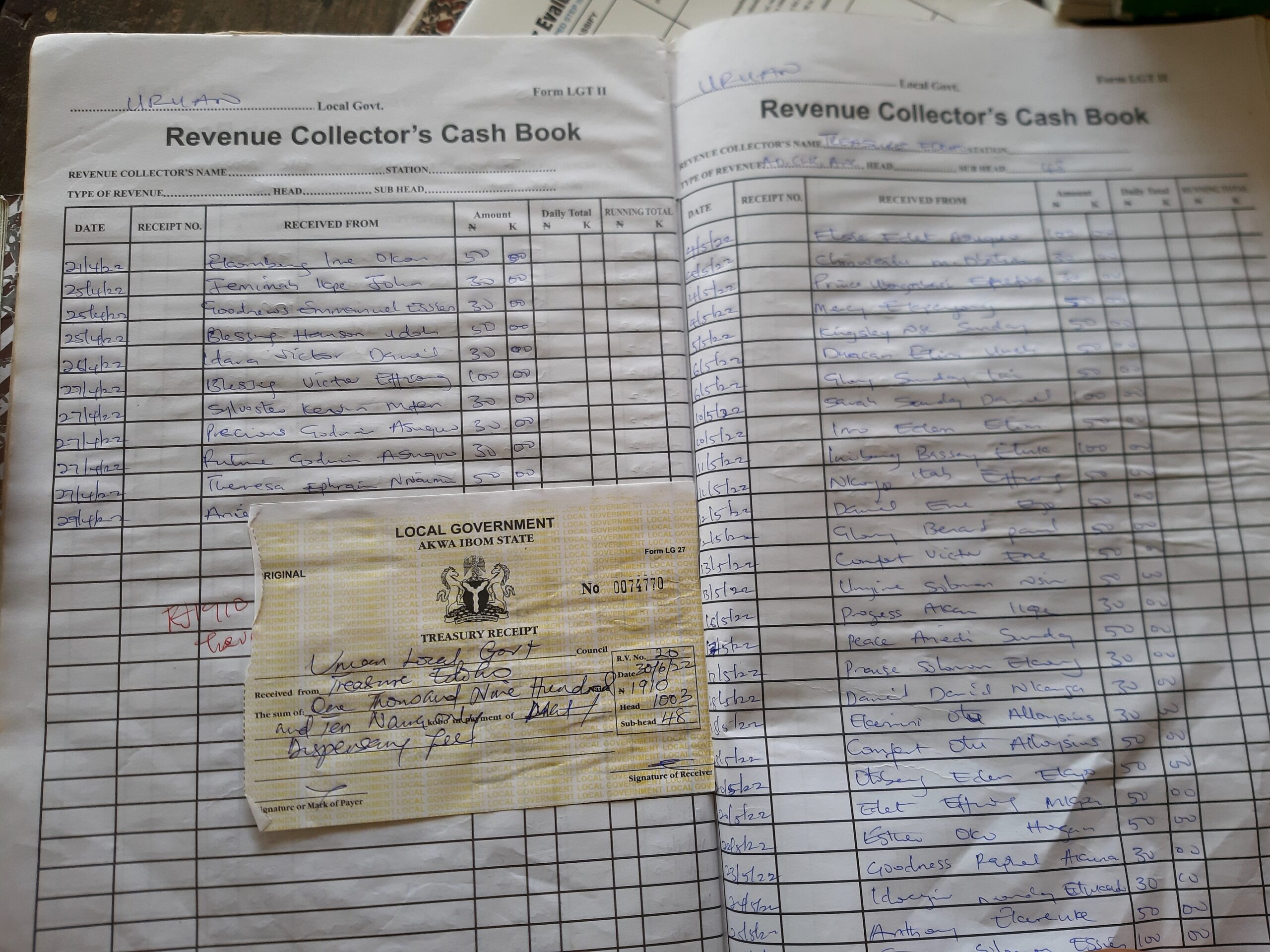
Revenue collector’s registers seen by PREMIUM TIMES showed evidence of revenue payment by PHCs across the state. For instance, between April and June 2022, PHC Nwaniba remitted ₦5,070 to the Uruan LGA and ₦1,910 in July. In August 2022, Essien Udim LGA received ₦4,050 as revenue from PHC Odoro Ikot.
The story is largely the same in all the PHCs across the five LGAs visited.
PREMIUM TIMES also found that despite these tax payments, PHCs receive no support from LGA councils in form of imprest or subventions to assist the facilities for better service delivery. Instead, staff often rely on personal contributions and sometimes donations from kind-hearted members of communities to run the facilities.

We are doing our best — Govt
The Chairman of the Akwa Ibom State Primary Healthcare Development Agency (AKSPHCDA), Martins Akpan, said the poor state of the PHCs stems from years of neglect under the control of the LGAs. He said the state governor, Mr Emmanuel, was doing his best to revive the primary healthcare system in the state to deliver quality healthcare to citizens.
“We must recognise the fact that these problems did not just start overnight. It is a product of neglect over the years. We just have to be thankful to the current governor, Deacon Udom Emmanuel, who has given visibility to the primary healthcare sector. Before now the PHCs were under the local government system. Everything was in shambles.
“It was just a couple of years ago that the FG decided to enact the National Health Act, which shifted the responsibility of the PHCs from LGAs to the state government under the provision of the Primary Health Care Under One Roof (PHCUOR). We are still in the process of the migration from the Local Government Service Commission to the state agency which will take care of these problems,” he said.
Mr Akpan said that plans were underway by the state government to engage quality health personnel to address the issue of staff shortage.
Addressing the issue of inequitable selection of PHCs, he revealed that the AKSPHCDA was not involved in the selection of the beneficiary PHCs, but noted that the PHCs that were not previously captured, especially the most affected ones, will be considered in the second phase.
While Akwa Ibom currently enjoys its share of 45 per cent of the BHCPF, the state is yet to access funds from the 50 per cent NHIS gateway meant for the provision of Basic Minimum Package of Health Services (BMPHS) to citizens, following the failure of the government to provide counterpart funding and the establishment of a health insurance agency. However, Mr Akpan assures that that would soon be a thing of the past.
“Health insurance is a part of the BHCPF. Now we have 45 per cent (NPHCDA gateway), we still need the 50 per cent which is even more than what we have already and you know his excellency (the state governor) understands and is working on it. I think what is left now is the nitty-gritty of setting up the agency so that they can have their own board and management,” he said.
*This report is supported by the International Budget Partnership and the International Centre for Investigative Reporting (The ICIR)
PREMIUM TIMES